Peer Review: Exploring the Landscape of Healthy Active Living Programming for School-aged Children in Newfoundland

Previously published in Volume 83, Issue 3
Abstract
Negative health trends in school-aged children are a growing concern in Canada. In response, there has been increased interest in healthy active living (HAL) programming targeting school-aged children, but to date such efforts have shown minimal impact. Research suggests that a significant number of youth still aren’t engaging in enough healthy behaviours to support optimal development for lifelong health and wellbeing. More knowledge about the types of HAL programming being offered across regions and provinces is urgently needed and could help better inform future directions in HAL programming. This qualitative research explored HAL programming in Newfoundland, Canada through a sequential mixed-methods study design. The study included focus groups and a survey tool to understand how individuals and communities in Newfoundland define HAL and what types of programming are being offered. Many organizations and stakeholders will benefit from understanding the gaps and opportunities for HAL programming. As presented here, the results of this research could help inform future research projects, as well as future community, regional, and provincial HAL strategies and programming.
Negative health trends in school-aged children [1] are a growing concern in Canada. Active Healthy Kids Canada (2016) report that youth aren’t engaging in enough positive healthy active living behaviours (i.e., physical activity, healthy eating, healthy sleep) to support optimal development for lifelong health and wellbeing. In response, there has been increased interest in healthy active living (HAL) programming targeting school-aged children, but to date such efforts have shown minimal impact. Despite the focus on HAL, research has shown that health outcomes for Canadian children are still a concern, and although they are well versed in healthy living discourse, they are choosing not to engage in healthy behaviours (Burrows, Wright, & Jungersen-Smith, 2002; Rail, 2009). More knowledge about the types of HAL programming being offered regionally, provincially and nationally could help to address potential gaps and opportunities and may improve health attitudes and behaviours. In turn, this awareness could provide essential insights for HAL decision makers, leaders, and facilitators to ensure programming is child-focused, comprehensive, evidence-based and wellness oriented.
The government of Newfoundland and Labrador (NL) has made it a priority to support people and communities to achieve lifelong health through initiatives such as the Provincial Wellness Plan, Healthy Students-Healthy Schools, Go Healthy: After-School Physical Activity Initiative, and Active, Healthy Newfoundland: A Recreation and Sport Strategy. While supporting communities to develop and implement HAL programs for school-aged children was a key target for NL’s healthy active living strategies, they realized the challenge to coordinate these programs effectively and understand the impact these initiatives have on health, learning and performance outcomes. To address this challenge, a university-government partnership was formed with the goal of better understanding the landscape of HAL in Newfoundland [2]. As such, the objectives of this study were to:
- understand the HAL discourse in programming targeting school-aged children;
- gather information on HAL initiatives, programs and activities;
- identify barriers, challenges, opportunities for HAL programming.
This study aspires to serve as an example for future research projects and inspire individuals and communities to explore new ways to deliver HAL programming that better meets the needs and realities of children today.
Research design
To achieve the objectives of the study, an exploratory sequential mixed-methods research design was employed (Creswell & Clark, 2007). After receiving ethical approval, the research team organized and hosted three focus groups in February of 2015 in three densely populated locations across Newfoundland: (1) St. John’s, (2) Corner Brook and (3) Gander. With a metropolitan area population of 205,955, St. John's was chosen because it is the capital of NL and the most easterly city on the island. Corner Brook was also chosen as a research site given that it has the second-largest population in Newfoundland at 19,806 and is located on the west coast of the island. The third site was chosen for its central location and larger population of 11, 688.
Purposive sampling via professional email was used to invite a total of 37 key community representatives from the sectors of education, public health, health services, sport and recreation. The focus groups were a full day in length and utilized various facilitation strategies (e.g., think-pair-share, world café, post-it notes, fill-in the blanks) to get as much information as possible about local HAL programming (i.e., initiatives, programs and activities). In these focus groups, representatives discussed the types of programming currently available to school-aged children, the types of populations and numbers served by these programs, the types of people running these programs, and how programs are being evaluated for effectiveness. Once focus groups were completed, data was transcribed from participants’ notes and chart paper into a spreadsheet. This information was then condensed and distributed to participants for member checking. A thematic analysis approach using Lichtman’s (2010) “Three C’s Analysis Approach” (Coding, Categorizing, Concepts) was used to identify key themes in the data. For this, data were coded and analyzed by two different members of the research team to ensure reliability of codes was upheld.
The focus groups helped to provide a more in-depth understanding of HAL discourses and programming in Newfoundland and informed the development of a survey tool. The survey reflected what was learned in the focus groups, with the goal of gathering more information from a wider audience. For this survey, participants were recruited through snowball sampling. A strategic recruitment strategy was developed to ensure that all communication channels were engaged, particularly through, email, media and social media channels. The link to the electronic survey (SurveyMonkey) was provided in emails, media releases, social media posts (e.g., Facebook, Twitter), and posted on websites (e.g. Memorial University’s School of Human Kinetics and Recreation). In total, 500 people participated from various regions across Newfoundland. The survey was designed and pilot tested several weeks before the final version was released. The survey availability lasted for two weeks, from April 13th to 26th, 2015. Once data collection was completed, all analyses were conducted using SPSS version 22. The survey focused on collecting demographic information, facilities and venues, HAL descriptions and programs, program types, key people, funding, evaluation, challenges, improvement and strengths. Frequencies and percentage of responses were calculated from respondents. Triangulation occurred after the survey data was collected to ensure that both the data from the focus groups and the survey were congruent.
Results
The results framed the three objectives of the study. First, the participants highlighted how they defined and characterized HAL. This section helped us to better understand the HAL discourse. Second, participants shared detailed information about HAL programming being offered in Newfoundland. Key insights related to the types, leaders, funding and evaluations are shared. Lastly, participants offered important insights for future directions in HAL programming in Newfoundland.
Healthy active living discourse
Defining HAL. During the focus groups, participants were asked how they would characterize or define HAL. Throughout the focus group discussions, participants emphasized two main ideas: holistic and lifestyle-oriented. Participants felt that historically there had been more focus on the physical dimension, but that now there is more of a focus on holism or wholeness—a balance of all the dimensions of an individual (i.e., mental, physical, emotional, spiritual)—as well as a balance in the programming between physical activity, healthy eating and mental well-being. Participants explained that HAL was focused on health promotion not disease prevention. When asked about the meaning of HAL, respondents from different locations across Newfoundland shared:
- Participant from St. John’s: “Healthy active living is about the social, emotional, physical, mental, cognitive.”
- Participant from Gander: “Activities that increase emotional, physical, healthy eating, socialization in everyday life.”
- Participant from Corner Brook: “Encouraging healthy eating, physical activity and positive mental health. Needs to be a collaborative effort between schools, community groups, organizations with support from parents.”
Participants also described HAL as being lifestyle-oriented, a way of life, where individuals make healthy choices a priority. Some participants explained that HAL is a culture, a mindset, and a day-to-day way of living. According to one of the participants from Gander, they stated, “It is a lifestyle rather than a bunch of scheduled activities or a diet.” Similarly one of the participants from Corner Brook said, “Healthy active living [is] lifelong, a mindset.” The ideology of lifelong living was put simply by a St. John’s participant. “Should be as simple as putting on a pair of socks, it's a lifestyle that should be naturally ingrained into everyone’s lives, families.”
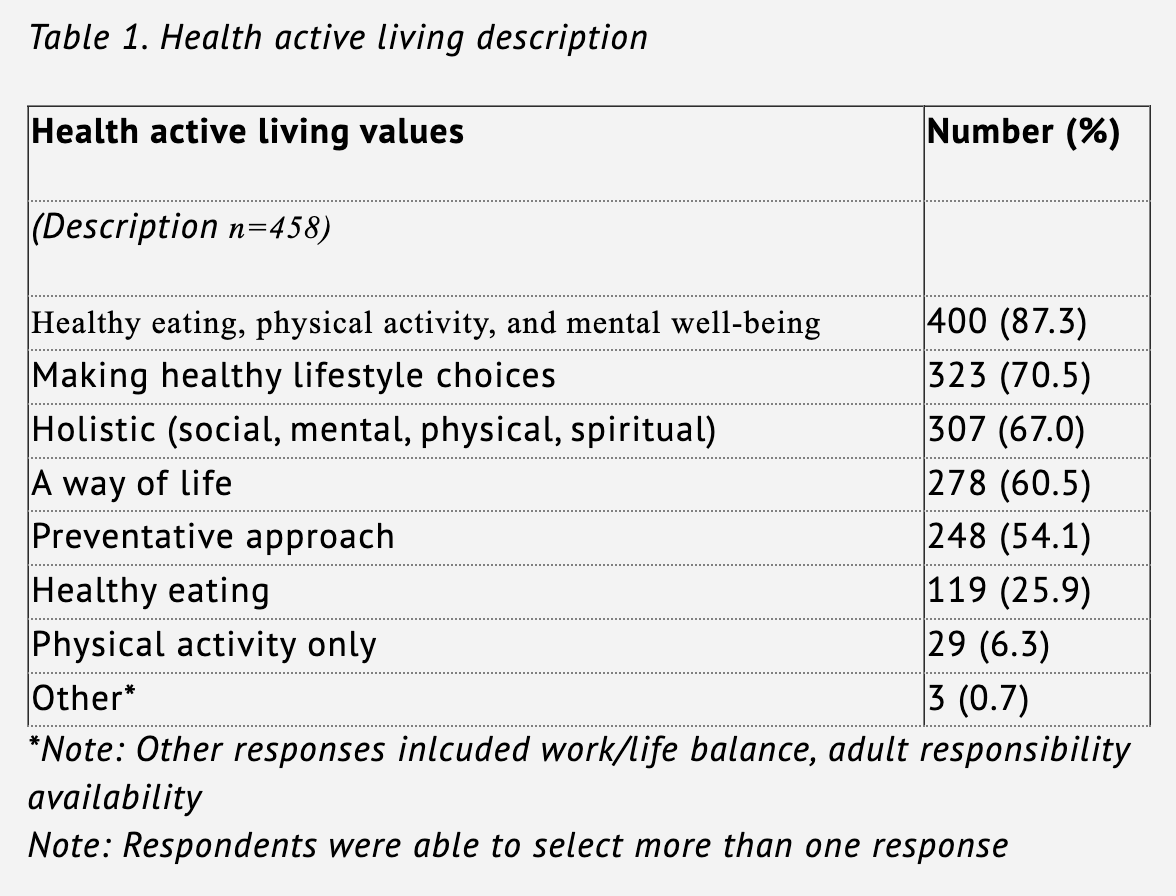
These perspectives were further supported by the survey results where the majority of respondents identified that HAL included healthy eating, physical activity and mental well-being (87.3%), rather than only one or the other. Respondents also identified that making healthy lifestyle choices (70.5%) and a holistic approach, including social, mental, physical, and spiritual aspects (67.0%) were important. Table 1 summarizes how survey respondents defined HAL.
Elements of HAL Programs. After defining HAL, focus group participants began to describe the nature of HAL programs for school-aged children in Newfoundland. Participants elaborated on their definitions of HAL and identified three key elements they felt were essential for HAL programs, namely: (1) accessibility, (2) affordability, and (3) inclusionary.
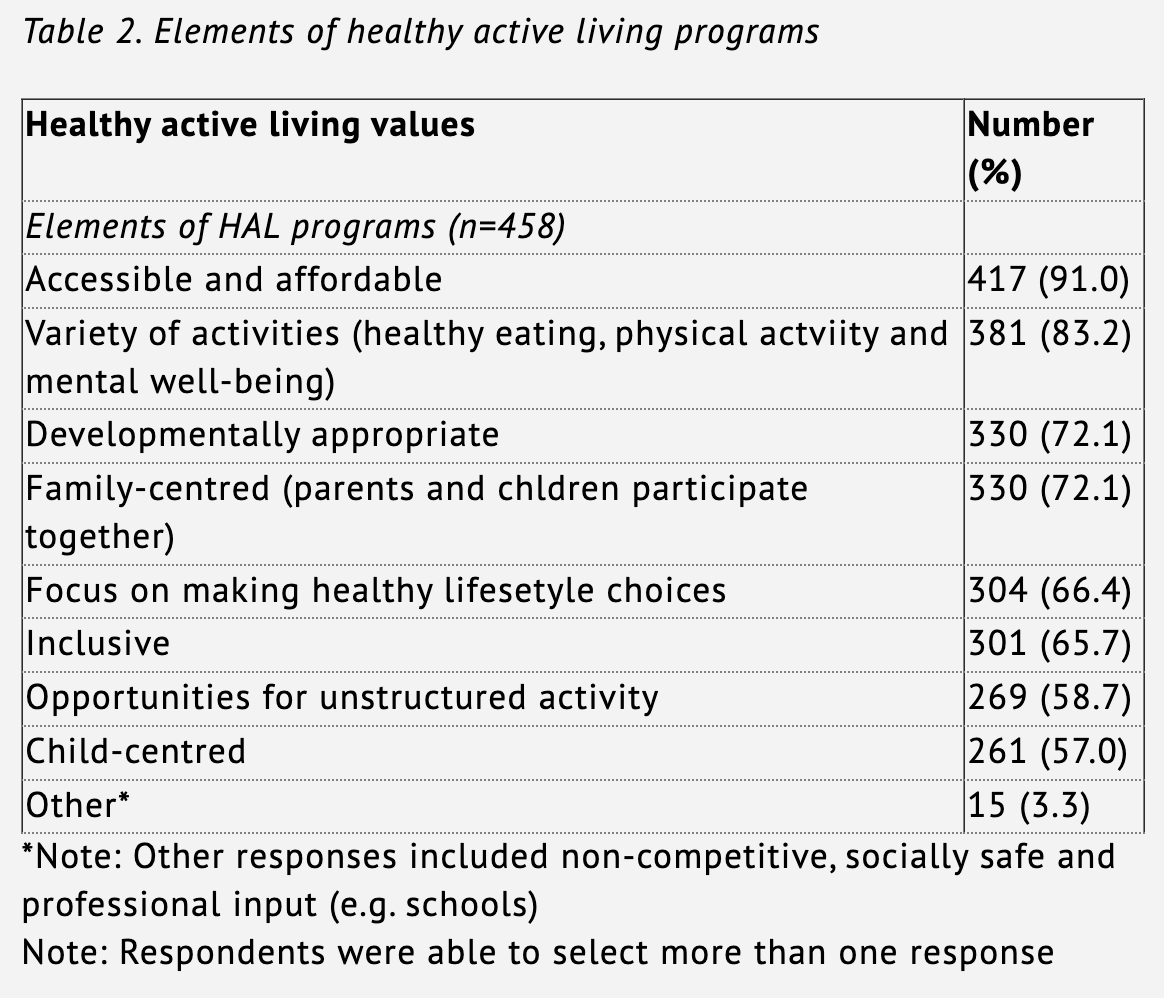
The results from the survey supported the findings from the focus group. Overwhelmingly, survey respondents (91.0%) identified that accessibility and affordability in HAL programs were of the upmost importance for youth. Additionally, respondents felt HAL programs should include a variety of activities, such as healthy eating, physical activity, and mental well-being (83.2%). Family-centered programming was also identified as being an essential element (72.1%), as these types of programs would allow parents to participate with their children. Table 2 summarizes how survey respondents’ prioritized the key elements of HAL programming for school-aged children.
Healthy active living programming
Types Of Programs. In the focus groups, participants identified specific HAL programs for school-aged children offered in their communities. Participants shared valuable information about programs such as the name, description, who was involved in offering the program, funding information and any evaluation information if known. Participants provided an understanding of the wide variety of programs available for school-aged children in Newfoundland. The types of programs that were highlighted by participants included community-based (e.g., Girl Guides of Canada; Scouts of Canada), school-based, nutrition-healthy eating (e.g. Breakfast Clubs), fitness, sport, targeted populations (e.g., girls-only, special Olympics), physical activity and private business/organizations (e.g. local ice hockey, ball hockey, swimming).
Participants identified that the majority of HAL programs offered in Newfoundland communities are physical activity related, specifically sport was discussed most often. Non-competitive physical activity, recreation and outdoor activity programs were also identified but not as frequently as sport. While a wide variety of HAL programs were identified, participants suggested a gap in programming related to healthy eating and mental health.
Survey results echoed the findings of the focus groups. When asked what types of programs are available for youth in their communities, survey respondents suggested that organized sport (85.5%), followed by community-based programming (70.2%), and outdoor recreation (59.8%) occur either frequently or very frequently. In contrast, very few participants listed mental health focused programs (13.2%), nutrition-based programs (19.3%), and one-time events (32.7%) as very frequently or frequently occurring programs.
Program Leaders. Focus group participants were asked about the people that deliver HAL programs across Newfoundland. As participants listed specific programs, they identified key coordinators and facilitators of HAL programs for school-aged children. Three types of key leaders were identified: (1) paid staff, (2) volunteers, and (3) specific individual champions. Programs that are facilitated by paid staff are those that are government funded, or offered by schools, health authorities, sport organizations, recreation centres and private businesses. This suggests that the personnel who set up and deliver the program are either full or part-time employees or contract personnel of those particular sectors (e.g., School District employees, recreation directors, private dance studio instructors). This also includes paid coaches from private sport organizations and studios. When survey respondents were asked who the key people are that run HAL programs for children in their communities, they indicated overwhelmingly volunteers (including coaches) were the most common leaders in the province. Specifically, participants mentioned student-volunteers, parents, coaches and community members as being the key leaders in running HAL programs for school-aged children.
Funding. The focus group participants identified two main sources of funding for communities in their efforts to support programming for young people: (1) grants (government and private corporation), and (2) fee-based structures. Participants suggested that many programs are offered in communities through nationally or provincially-based programs (e.g. ParticipACTION, Participation Nation). While, other programs rely upon federal, provincial and municipal government grant funding that individuals and organizations must apply for (e.g. Public Health Agency of Canada, Wellness Fund). As referred to by many of the participants, many local programs are private in nature and have costs associated for families wishing to participate. Reference was made by participants to programs that are funded by partner corporations, such as Jumpstart (Canadian Tire) and Kraft Celebration grants to help reduce these costs for registration and programming fees.
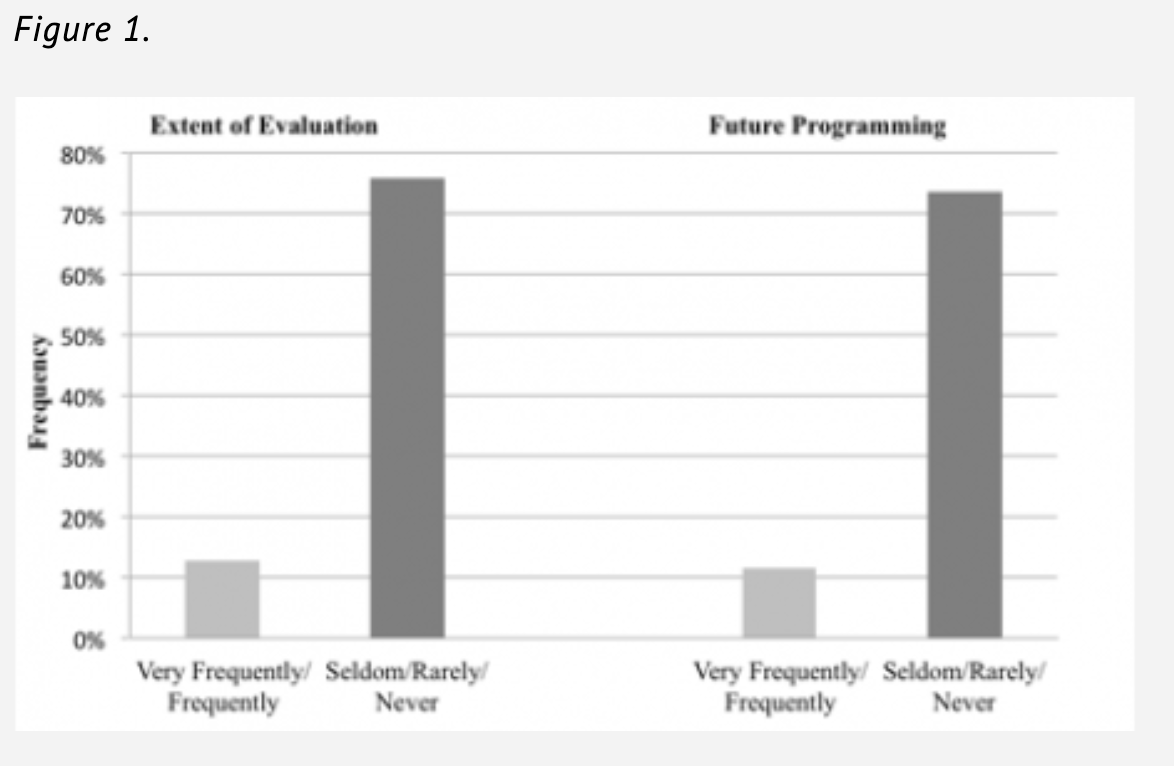
Program Evaluation. Focus group participants and survey respondents both suggested that programs in Newfoundland were seldom or rarely evaluated for their effectiveness. As seen in Figure 1, for those programs that are evaluated, results seldom or rarely inform future programming. When asked what indicators should be evaluated, level of enjoyment (88.9%), individual health measures (87.3%), and social-emotional (76.7%) factors were listed most frequently. Fewer respondents suggested that evaluation should be focused on fundamental movement skills (49.6%), or sport-based skills (40.5%). Very few respondents (1.8%) suggested that an evaluation is not necessary.
Future of healthy active living programs
The final section provides insights into the future of HAL programming in Newfoundland. In the study, focus group participants and survey respondents were asked to articulate the strengths, opportunities and challenges of HAL programming for school-aged children. While participants discussed these three different perspectives separately, there were many similarities and complexities. The following section highlights the four key ideas identified: (1) resources, (2) infrastructure, (3) programming, and (4) culture.
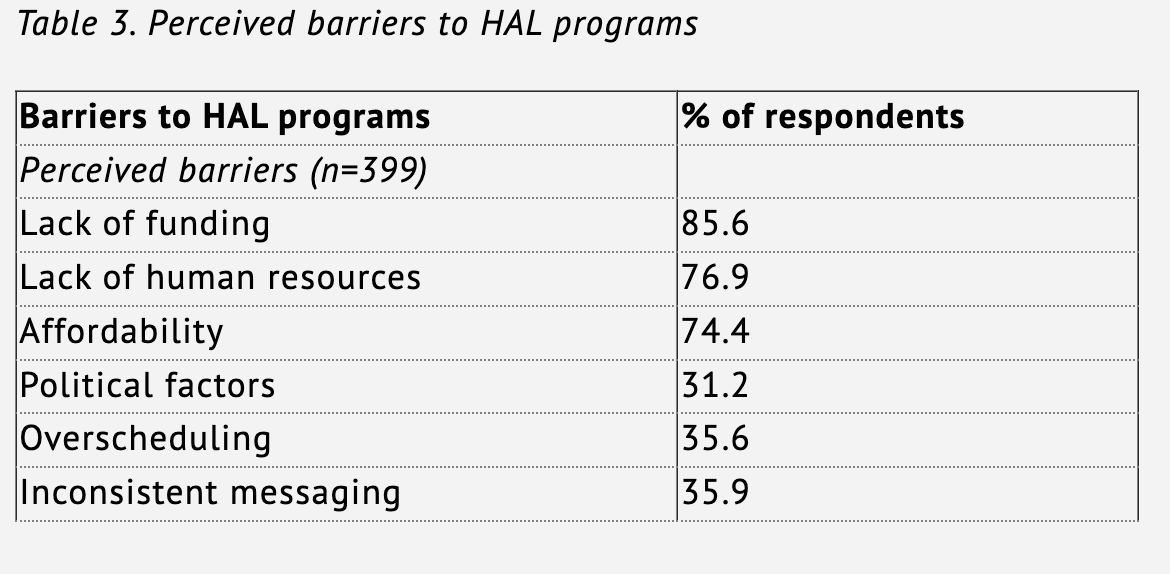
Resources. Participants spoke about various resources, particularly in the areas of funding, people, support, technology, and volunteers. One of the participants stated, “[We] have community champions, volunteers and teachers that give back to community.” While resources were identified as a strength, particularly from participants in Gander and Corner Brook, they were also framed as a barrier and an important area to address in future healthy active living programs. Participants felt that increased resources for HAL could make programs better. They suggested that there is limited funding, people, and support to provide healthy active living programs for children and youth. This was reinforced through the survey respondents, as evidenced in Table 3.
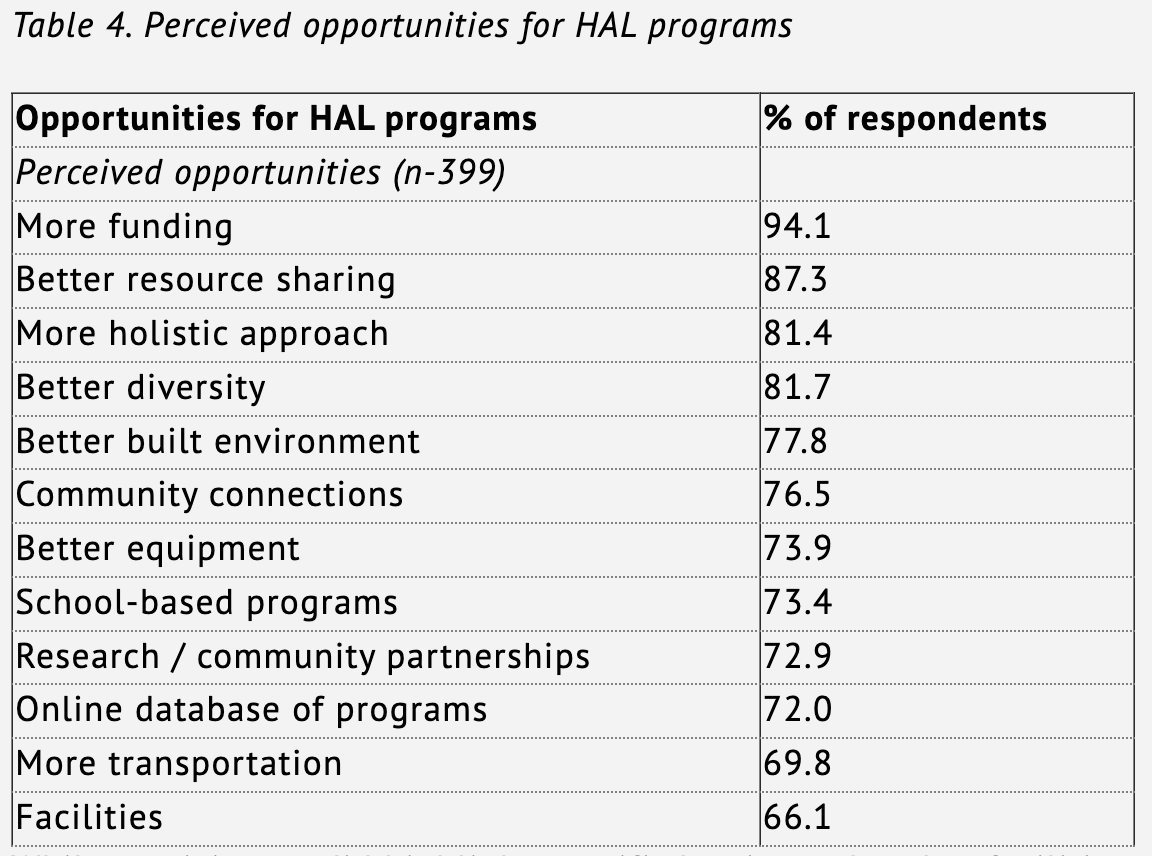
Other ideas suggested from the focus groups participants included developing a database of available programs, increasing research capacity and knowledge translation in the province, increasing general and targeting funding with evaluative components, and increasing support from people in Newfoundland. According to one of the participants from Corner Brook, “We need a database of all activities available and facilities: good for new people to province to see what’s offered.” Similarly one of the participants from St. John’s stated, “We have fabulous programs out there but we need to make the connections with them.” The focus groups recognized the strengths associated with their individual programs but emphasized the necessity for collaboration with other groups. Better resource sharing was identified as a key opportunity for improving future HAL programming, as seen in Table 4.
While participants did highlight specific barriers related to facilities and equipment for HAL programming, they also spoke about existing strengths within their communities. Some participants suggested that there are already adequate equipment, facilities, venues, and outdoor areas available to promote HAL for children in the province. In fact, there was sense of pride in the responses by participants when talking about existing community centers and schools that are used for healthy active living programming. Interestingly, there was also more of an emphasis from Corner Brook and Gander participants than St. John’s related to the importance of the outdoors for healthy active living. Participants clearly recognized the beauty in their surrounding landscape and how communities can take advantage of this to lead healthy and active lifestyles. As stated by a participant from Corner Brook, the “use of the outdoors in our programming plays a big role in the active lifestyle here.” With that said, participants suggested that improving infrastructure within Newfoundland could have a positive impact on children in the province. They suggested the need for special attention towards improving accessibility and transportation to and from places. Participants also suggested that advocacy for updating facilities and improving outdoor spaces should be a priority.
Programming. Many participants discussed that a strength of current HAL programs is how they are run. This includes scheduling, breadth of activities, access to activities, and school-based programming (emphasized by Corner Brook and Gander participants). What was also evident from both the focus groups participants and survey respondents is that a significant number of HAL programs are available to children in Newfoundland.
In the focus groups alone, St. John’s participants identified 135 different programs, Gander listed 92 programs, and Corner Brook highlighted 86 programs. Further, participants discussed a number of opportunities to improve programming in Newfoundland. Firstly, there could be more activities introduced in a wider variety of formats. Secondly, schools already play an important role across the province so there is a need to support schools. Lastly, participants also discussed key opportunities and the need for more evaluation and professional development. While there were many strengths discussed with regards to programming, participants also suggested on numerous occasions that the way programs were conducted and governed was a barrier to HAL in Newfoundland. According to one of the participants, some issues are out of their control. “Lack of long term planning due to changing governments [is a challenge].” Some of the additional barriers mentioned by participants included: program structure, scheduling, programs, transportation, implementations, connections, and breadth.
Healthy Active Living Culture. Broadly speaking, participants suggested culture refers to the connection between people and the messaging about the importance of HAL. Focus group participants suggested that HAL culture was stronger in Corner Brook and Gander because in small communities there is more potential to impact HAL, as people often feel more connected to each other. Participants also suggested they can prioritize what needs to be done and place value towards certain aspects of HAL programming.
Participants also suggested that there should be more opportunities to create a HAL culture in communities. Participants suggested opportunities to improve HAL culture included: (1) better access to programs, (2) more equal access,(3) a larger breadth of programs, (4) more community connections, (5) various opportunities based on geography, (6) a more holistic approach and (7) a more inclusive environment. It is also important to note that Corner Brook and Gander participants knew their communities so well that they felt they knew exactly what they needed to better meet the needs of all youth.
While there was a strong sense of HAL culture in the focus groups, culture was also identified as a barrier. Many participants suggested that there was not enough, a lack of, and inconsistent communication related to HAL programs. According to one of the members of the St. John’s focus group, “Need more interaction with healthy active living for people to learn about what each of us are doing and to find ways to work together.” Participants identified a lack of priority in families, communities and government (time), tenuous politics that shift with new leadership, fear of engaging in HAL programming (liability), limited promotion surrounding the benefits of healthy active living, and, limited engagement with HAL-related education, evidence, and evaluation as examples of cultural barriers.
Finally, both the focus group participants and the survey respondents outlined a strong desire for wanting HAL programming to grow and evolve in the province. They also highlighted the benefit of participating in this research study. According to one of the participants from Gander, “It is great to know that we are all concerned. [I like the] opportunity to discuss about things happening in the province…sometimes we get stuck in our own region.” The focus group participants, in particular, saw the focus groups as a chance to collaborate and meet with other colleagues in the area. According to one of the participants from Corner Brook, “[It was good to have] the opportunity to be heard and collaborate with other professionals...to collaborate with members of other groups, i.e. health field, government service.”
Recommendations
This study not only provided insights about HAL programming for school-aged children, but also initiated conversations among and across sectors, and opportunities for new connections between university researchers, governments, and community partners. The results of this study provide valuable insights for bringing research-to-practice and practice-to-research. It highlights how HAL is being defined, what HAL programming is being offered, and future directions for HAL in Newfoundland. This final section discusses the findings in relation to existing literature and presents recommendations for HAL programming in Newfoundland.
Healthy discourse: Aligning definitions and practice
Participants in this study defined HAL as holistic in nature, focusing on all the dimensions of health—physical, mental, emotional, spiritual. As a result, they felt that HAL programming must reflect this understanding and include a balance of physical activity, mental well-being, and healthy eating. However, when they discussed the types of programs being offered in their communities, most if not all, focused on the physical. A gap between what is conceptualized and what is practiced, was noted. Additional funding for comprehensive approaches to HAL programs may improve the current compartmentalized approach that is prevalent across the province. As noted by Veugelers and Schwartz (2010), efforts to optimize children’s health outcomes are often impeded by the complexities and lack of clarity in implementing holistic health. However, researchers have noted that when emphasis is put on health and wellness (e.g., Nova Scotia’s Annapolis Valley Health Promoting Schools Project and Alberta’s APPLE Schools) the comprehensive approach to HAL begins to merge healthy eating, mental health and physical activity (Bassett-Gunter, Yessuis, Manske, & Gleddie, 2016, Fung at al, 2012; Vander Ploeg et al., 2014).
HAL programming: Creating volunteer sustainability
Participants in this study identified that HAL programming would not be possible without the many volunteers who dedicate their time. In Canada, 2 million volunteers serve as youth sport coaches (Coaching Association of Canada, 2007). Volunteering is a pivotal human resource in the community sport and recreation sector and important in creating opportunities for children (Harman & Doherty, 2014). Program leaders not only allow for the children to experience sport, but they also influence children’s psychosocial development (Petitpas, Cornelius, Van Raalte, & Jones, 2005). In many communities, sport programs are often non-profit, voluntarily managed and member-driven by champions within the community. Every community has champions who consistently volunteer to organize and facilitate a variety of physical activity programs. While this is positive news, participants warned about trends of burnout and declining volunteer activity. Research on volunteering has shown that volunteer positions are becoming difficult to fill and there is a low rate of champion retention (Cuskelly et al., 2006; Gumulka, Barr, Lasby, Brownlee, 2005; Paiement, 2007). Therefore, the province needs to work together with communities to consider how to sustain programming, while promoting a holistic approach. An awareness that support, training, recognition, updated information, contemporary techniques and evidence-based professional development for program leaders will become increasingly important if a holistic lifestyle approach is to be achieved.
Strategic funding and collaboration: Addressing complexity
The results indicated that most HAL programs are fee-based. This presents significant financial barriers for many families across Newfoundland. Participants also commented on transportation costs for getting to and from facilities as a barrier to participation. It is well-known that socio-economic status is related to physical activity participation, thus a better understanding of the barriers faced by lower socio-economic segments of the population is crucial for developing new strategies and initiatives (Drenowatz et al, 2010; Humbert et al., 2006; Veselska, Geckova, Reijneveld & vanDijk, 2011). Some researchers suggest that comprehensive, multilevel programming targeting physical activity behaviours, social and physical environments, as well as other psychosocial considerations are needed (Cerin & Leslie, 2008; Veselska, Geckova, Reijneveld & vanDijk, 2011). Program access and affordability will need to be reviewed to better support HAL programming in all communities.
An interesting paradox emerged when asking study participants about the strengths, opportunities and challenges associated with HAL programs for school-aged youth. On one hand, community members identified many improvements that are needed with regards to funding, resources, expertise, culture and partnerships. On the other hand, participants were very proud and appreciative of what is being offered in their communities. Overall, the study illustrates the complexity of HAL programming, which suggests that all future HAL programs, initiatives, and activities need to be addressed in a more comprehensive way.
Researchers have recommended strategic collaborations between programs. Baker, Ansari, and Crone (2017) have referred to uncoordinated community networks as “silos” (p. 88) where community groups are not working simultaneously to ensure efficiency and effectiveness. According to Rowe et al. (2013), “it is imperative that all stakeholders, policy makers, and researchers alike, recognize the value in bringing together sport performance, community, and health-oriented agendas” (p. 375). As seen in this study, at the community level there is the silo effect, where collaboration will not only improve resource development but also foster community partnerships in creating a more holistic nature to HAL programming in Newfoundland.
Conclusion
This study suggests that a multi-level, collaborative strategy for school-aged HAL programming would be beneficial in NL. Such a strategy would ensure that a more interconnected approach was taken to promoting HAL for children and building a culture of HAL in the province. A strategy of this nature would include collaboration with community and organizations to meet the government-wide wellness priorities that include all dimensions—mental, physical, emotional, and spiritual. Partner organizations, university researchers and community members would be important partners in this initiative to ensure action items are appropriate to the goals.
-
School-aged children refers to children and youth in the age range of 5 to 17 years of age.
-
Note: This study focused on the island portion of Newfoundland and Labrador only. A subsequent study focused on Labrador has since been completed to provide a full provincial perspective.
References
Active Healthy Kids Canada. (2008). Canada’s report card on physical activity for children and youth – 2007. Retrieved from http://www.jeunesenforme.ca/programs_2007reportcard. cfm.
Bassett-Gunter, R., Yessis, J., Manske, S., & Gleddie, D. (2016). Healthy school communities in Canada. Health Education Journal, 75, 235-248.
Burrows, L., Wright, J., & Jungersen-Smith, J. (2002). “Measure your belly.” New Zealand children’s constructions of health and fitness. Journal of Teaching in Physical Education, 22, 39-48.
Canadian Mental Health Association (2015). Fast facts about mental illness. Retrieved from http://www.cmha.ca/media/fast-facts-about-mental-illness/#.VWcB1mRVikp
Cerin, E., & Leslie, E. (2008). How socio-economic status contributes to participation in leisure-time physical activity. Social Science and Medicine, 66(12), 2596-2609.
Coaching Association of Canada. (2007). News release. Volunteer coaches essential to Canadian sport. Ottawa: Canada.
Colley, R. C., Garriguet, D., Janssen, I., Craig, C. L., Clarke, J., Tremblay, M. S. (2011). Physical activity of Canadian children and youth: accelerometer results from the 2007 to 2009 Canadian Health Measures Survey. Health Reports, 22, 15–23.
Creswell, J. (2007). Qualitative inquiry and research design: Choosing among five approaches. Thousand Oaks, CA: Sage.
Creswell, J. W., & Clark, V. L. P. (2007). Designing and conducting mixed methods research. Thousand Oaks, CA: Sage.
Cuskelly, G., Taylor, T., Hoye, R., & Darcy, S. (2006). Volunteer management practices and volunteer retention: A human resource management approach, Sport Management Review, 9, 141-163.
Drenowatz, C., Eisenmann, J. C., Pfeiffer, K. A., Welk, G., Heelan, K., Gentile, D., & Walsh, D. (2010). Influence of socio-economic status on habitual physical activity and sedentary behavior in 8-to 11-year old children. BMC Public Health, 10(1), 214.
Fung, C., Lu, C., Kuhle, S., Prcell, M., Schwartz, M., Storey, K. (2012). From ‘best practice’ to ‘next practice’: he effectiveness of school-based health promotion in improving healthy eating and physical activity and preventing childhood obesity. International Journal of Behavioral Nutrition and Physical Activity, 9, 27, 1-9.
Graham, P., Evitts, T., & Thomas-MacLean, R. (2008). Environmental scans: How useful are they for primary care research? Canadian Family Physician, 54(7), 1022-1023.
Greene, M. (1995). Releasing the imagination: Essays on education, the arts and social change. San Francisco: Jossey-Bass.
Gumulka, G., Barr, C., Lasby, D.,& Brownlee, B. (2005). Understanding the capacity of sports and recreation organizations: A synthesis of findings from the National survey of nonprofit and voluntary organizations and the national survey of giving, volunteering and participating [Image Canada website]. Retrieved from http://sectorsource.ca/sites/default/files/resources/files/understanding_capacity_of_sport_rec_report.pdf
Harman, A. & Doherty, A. (2014). The psychosocial contract of volunteer youth sport coaches. Journal of Sport Management, 28, 687-699.
Health and Education Research Group. (2008). Investigating positive psychology themes in school health: a scan and analysis of provincial/territorial education department websites. Retrieved from http://eng.jcsh-cces.ca/upload/ PositivePsychologyinSchoolsApril2009.pdf.
Humbert, M. L., Chad, K. E., Spink, K. S., Muhajarine, N., Anderson, K. D., Bruner, M.W., & Gryba, C. R. (2006). Factors that influence physical activity participation among high-and low-SES youth. Qualitative health research, 16(4), 467-483.
Kumar, S., Quinn, S., Kim, K., Musa, D., Hilyard, K., & Freimuth, V. (2012). The social ecological model as a framework for determinants of 2009 H1N1 influenza vaccine uptake in the US. Health Education Behaviour, 39, 229-243.
Lichtman, M. (2010). Qualitative research in education: A user’s guide. Thousand Oaks, CA: Sage Publications.
Morrison, W. & Kirby, P. (2012). Schools as a setting for promoting positive mental health: better practices and perspectives. Retrieved from http://eng.jcshcces.ca/upload/JCSH%20Positive%20Mental%20Health%20Lit%20Review%20Mar%22010.pdf.
Paiment, C. (2007). Youth sport coaches: Factors that predict satisfaction with the coaching experience, Research Quarterly for Exercise & Sport, 78
Park, S., Sappenfield, W. M., Huang, Y., Sherry, B., & Bensyl, D. M. (2010). The impact of the availability of school vending machines on eating behavior during lunch: the Youth Physical Activity and Nutrition Survey. Journal of American Dietetic Association, 110,1532–1536.
Petipas, A., Cornelius, A., Van Raalte, J., & Jones, T. (2005). A framework for planning youth sport programs that foster psychosocial development. The Sport Psychologist, 19, 63-80.
Public Health Agency of Canada. (2008). Canada’s physical activity guide to healthy active living. Retrieved from http://www.phac-aspc.gc.ca/pau-uap/paguide/child_youth/pdf/kids_family_guide_e.pdf.
Rail, G. (2009). Canadian youth’s discursive constructions of health in the context of obesity discourse. In J. Wright & V. Harwood (Eds.), Biopolitics and the ‘obesity epidemic’ (pp.142-156). New York, NY: Routledge.
Rodgers, S., Hibbert, K., Leschied, A., Pickle, L., Stepien, M., Atkins, M., Koening, A.,Woods, J., & Vandermeer, M. (2014). Shaping a mental health curriculum for Canada’s teacher education programs: Rationale and brief overview. Physical and Health Education Journal, 80.
Shields M. (2005). Nutrition: findings from the Canadian Community Health Survey. Measured obesity: overweight Canadian children and adolescents [Internet]. Chart 9: Overweight and obesity rates, by fruit and vegetable consumption, household population aged 2 to 17, Canada excluding territories, 2004. Retrieved from http://www.statcan.gc.ca/pub/82-620-m/2005001/c-g/child-enfant/4053588-eng.htm
Statistics Canada. (2011a). Body mass index of Canadian children and youth, 2009 to 2011. Health Fact Sheet. Retrieved from http://www.statcan.gc.ca/pub/82-625x/2012001/article/11712-eng.htm (1)
Statistics Canada. (2011b) Directly measured physical activity of Canadian children and youth, 2009 to 2011. Health Fact Sheet. Retrieved from http://www.statcan.gc.ca/pub/82625-x/2013001/article/11817-eng.htm (2)
Taber, D. R., Chriqui, J. F., Perna, F. M., Powell, L. M., & Chaloupka, F. J. (2012).Weight status among adolescents in States that govern competitive food nutrition content. Pediatrics, 130, 437–444.
Templeton, S.B., Marlette, M.A. & Panemangalore, M. (2005). Competitive foods increase the intake of energy and decrease the intake of certain nutrients by adolescents consuming school lunch. Journal of American Dietetic Association, 105, 215–220.
Trajkovski, S., Schmeid, V., Vickers, M., & Jackson, D. (2013). Using appreciative inquiry to transform health care. Contemporary Nurse, 45, 95-100.
Waddell, C. & Shepherd, C. (2002). Prevalence of mental disorders in children and youth: A research update prepared for the British Columbia Ministry of Children and Family Development. Vancouver mental health Evaluation and Community Consultation Unit.
Vander Ploeg, K., McGavock, J., Maximova, K., et al. (2014). School-based health promotion and physical activity during and after school hours. Pediatrics, 13, 2013-2383.
Veselska,Z., Geckova, A., Reijneveld, S. & vanDijk, J. (2011). Socio-economic status and physical activity among adolescents: The mediating role of self-esteem. Public Health, 125(11), 763-768.
Veugelers, P. & Schwartz, M. (2010). Comprehensive school health in Canada. Canadian Journal of Public Health, 101, 5-8.
Authors













