Are Ontario Secondary School Staff Trained and Supported in Delivering Healthy Eating and Weight-Related Initiatives?

Previously published in Volume 82, Issue 3
Abstract
This paper examines the professional development and support of school staff in the effective and safe delivery of healthy eating and weight-related initiatives. Representatives at 79 Ontario Secondary Schools in the COMPASS study (2012/2013; 2013/2014) completed surveys on school policies, resources, and staff training. Large disparities in resources (budget, support for staff time) allocated to schools for health promotion activities were evident. Staff at more than half of the participating schools had not been trained on nutrition (62.0%) or body image (54.4%) in the past year, with the most frequent form of nutrition training initiated by teachers and conducted on the internet. Results suggest calls to improve the education of school staff on weight-related issues have not been consistently answered. Increased efforts are advised to ensure educators are supported in delivering the new Health and Physical Education Curriculum, and continuing health promotion and obesity prevention efforts.
In response to the high prevalence of childhood and adolescent obesity (Tremblay et al., 2010), several school-based prevention programs and policies continue to be implemented (Public Health Ontario, 2013; Kropski, Keckley & Jensen, 2008). Schools have been identified as key settings for health promotion efforts as they provide continual access to the large majority of adolescents in Canada. However, considerable debate exists on whether some obesity prevention efforts may potentially be more harmful than beneficial. For instance, opponents have argued that addressing obesity in schools may promote poor body image, weight preoccupation, disordered eating, weight bias, and weight-related bullying (Carter & Bulik, 2008; Pinhas et al., 2013; Russel-Mayhew, McVey, Bardick & Ireland, 2012).
The effect of obesity prevention programs and related curriculum is likely contingent on the nutrition and weight-regulation knowledge and attitudes of the teachers responsible for their delivery. School staff are increasingly positioned to be healthy role models, ensure the physical wellness of their students, and incorporate health education components across the school curricula (Schee & Gard, 2014). While teachers appear willing and supportive of addressing childhood obesity in schools (Greenleaf, Martin & Rhea, 2008; Greenleaf & Weiller, 2005; Neumark-Sztainer, Story & Harris, 1999), whether they are equipped to fulfill this expectation has essentially been neglected (Neumark-Sztainer et al., 1999; Yager & O’Dea, 2005). To date, evaluation efforts have concentrated on program theory and content, with scant consideration of the competency and support of the teachers leading the curriculum (Yager, 2010; Yager & O’Dea, 2005).
Limited training, knowledge and support
Despite teachers wanting to take action, evidence from research examining the knowledge of nutrition, eating disorders, and obesity among prospective teachers is cause for concern (Greenleaf & Weiller, 2005; Sharma et al., 2013; Yager & O’Dea, 2005). Teachers themselves cite limited training, knowledge, and support as barriers to addressing weight-related issues, along with time and curricular constraints (Greenleaf & Weiller, 2005; Lister-Sharp, Chapman, Stewart-Brown & Sowden, 1999; Neumark-Sztainer et al., 1999; Snelling, Belson & Young, 2012; Yager & O’Dea, 2005); factors linked to less successful implementation of school-based health promotion programs (Neumark-Sztainer et al., 1999).
These findings are unsurprising considering the complexities of obesity and abundance of misinformation on nutrition and weight determinants currently available in the popular literature and online (Puhl & Heuer, 2010). In the absence of appropriate support and training, teachers’ knowledge cannot be expected to differ from the general public’s understanding of obesity, which tends to overemphasize personal responsibility (Puhl & Heuer, 2010). Indeed, research shows that many physical educators and trainees hold overly simplistic views on weight regulation, attributing obesity exclusively to excess caloric intake and inadequate physical activity, and failing to account for important genetic, biological, and social determinants of health (Greenleaf & Weiller, 2005; Yager, 2010).
Evidence of weight bias
Various experts fear these misconceptions may be transmitted to students, encouraging weight bias and weight-related bullying (Yager, 2010; Peterson, Puhl & Luedicke, 2012). Moreover, weight bias is evidenced among school staff. For instance, physical educators have been found to view heavier students more negatively than youth without excess weight (Greenleaf & Weiller, 2005; Peterson et al., 2012). In addition to conveying stigmatizing attitudes, educators may inadvertently model the weight/shape preoccupation and unhealthy weight-control behaviours that they are intended to prevent (Yager, 2010; Yager & O’Dea, 2005). Health and physical education teachers and teachers-in-training display elevated levels of body dissatisfaction, excessive exercise, dieting, and disordered eating behaviours (Chen et al., 2010; Yager & O’Dea, 2009), similar to professionals in other health-focused careers (e.g., nutritionists).
Researchers and policy makers recognize the potential risks, and have urged school administrators and boards to invest in the professional development of teachers in order to dispel common myths and ensure their influence is health promoting and not harmful (Pinhas et al., 2013; Russell-Mayhew et al., 2012; Yager, 2010; McVey, Tweed Ferrari, 2005; Ontario Ministry of Education, 2012). Likewise, key stakeholders at a recent Weight Bias Summit stressed the need to address gaps in teacher training on health and weight-related issues.20 The advised training extends past nutrition and exercise, to raise awareness of the factors contributing to body image development, eating disorders, and weight bias. Recommended interventions would sensitize staff to the adverse consequences of weight bias, ways in which weight bias appears, and allow reflections on their own views regarding health, food, and body weight (Pinhas et al., 2013; Russell-Mayhew et al., 2012; Yager, 2010; McVey et al., 2005).
Few body image programs available
Similar issues to those discussed regarding teacher-led obesity prevention initiatives are present for eating disorder prevention. The few disordered eating and body image programs that have been implemented in schools predominantly resulted as part of externally funded research projects, and were delivered by researchers (Yager, Diedrich, Ricciardelli & Halliwell, 2013; Yager & ODea, 2015). Moreover, programs that were led by teachers frequently deviated from intended content and were less effective (Yager et al., 2013; Yager & O’Dea, 2015). Educators themselves report feeling unconfident in selecting and delivering material on body image, and desire better resources and training (Yager et al., 2013; Yager & O’Dea, 2015). Instead, schools often address body image and eating disorders by inviting guest speakers who have experienced an eating disorder, an ill-advised method for primary prevention (Yager & O’Dea, 2015).
It remains unclear whether these calls for greater training have been answered. The resources available to educators in leading health curriculum and activities may have improved with the increasing focus on adolescent health behaviours and obesity prevention. In light of the recently revised Ontario health curriculum (2015), which emphasizes adequate teacher training and support, evaluating current preparedness to effectively and safely implement such programs is timely. Accordingly, this paper aims to provide a school-level perspective on the professional development and support of staff in delivering healthy eating and weight-related initiatives in a sample of Ontario secondary schools participating in the COMPASS study.

Methods
Design
COMPASS is a cohort study collecting hierarchical longitudinal data from a large sample of grade 9 to 12 students and the secondary schools they attend in Ontario and Alberta, Canada (Leatherdale et al., 2014). The current paper reports on the baseline school-level data from the 79 secondary schools in Ontario. A full description of the study methods is available in print (Leatherdale et al., 2014) or online (www.compass.uwaterloo.ca).
Data collection tools
Questions were drawn from the COMPASS School Programs and Policies Questionnaire (SPP), which is a paper-based survey designed to measure the presence/absence of relevant programs, practices, or resources within a school related to student health in multiple behavioural and risk factor domains. While the SPP was based on the previously validated Healthy School Planner (2014) tool, it was modified to be shorter (to improve school completion of the tool) and to cover additional content domains. Specific to this manuscript, the SPP assessed the frequency and type of teacher training and professional development on nutrition and body image, as well as whether staff had clear guidelines to appropriately refer students suspected of having eating disorders, school collaboration with local public health units and outside organizations, and budget and staff time allocated for health promotion activities by the school board or committee.
Sample/recruitment
In Year 1 (Y1: 2012-2013), 43 secondary schools were purposefully recruited to participate in the COMPASS study at which time they provided their baseline data. In Year 2 (Y2: 2013-2014), an additional 36 schools were also purposefully recruited to participate in the COMPASS study at which time they provided their baseline data. As described elsewhere (Thompson-Haile & Leatherdale, 2013; Bredin, Thompson-Haile & Leatherdale, 2015), eligible schools were approached after their board granted approval. Inclusion criteria required schools to be English-speaking secondary schools with students in grades 9 to 12. Schools also had to allow the use of active information-passive consent parental permission protocols (Leatherdale et al., 2014).
A variety of schools was represented, including 22 Eastern, 30 Southwestern, and 18 Northern Ontario schools, as well as 9 schools in the Greater Toronto Area. About 4% of the schools were from rural areas, and 39.2%, 17.7%, and 39.2% from large, medium, and small urban areas, respectively. School sizes ranged from 153 to 1400 enrolled students (Mean=756.3, standard deviation=284.7). The majority were from the Catholic (42) and public (31) school boards, and 6 were private schools.
The survey was completed by the school representative most knowledgeable about the program and policy environment within the school. For the majority of the schools this representative was a head administrator (i.e., Principal, Vice Principal, Superintendent, n=54), a member of the guidance/student services staff (including Student Success Teachers, n=12), or a physical education educator or department head (n=9). The remaining 4 surveys were completed by other teachers. COMPASS staff collected the completed surveys and followed up to verify the information provided.
The COMPASS study was approved by the University of Waterloo Office of Research Ethics and appropriate School Board committees.
Results
Support from school board to improve the health of students
Of the 79 schools surveyed, almost half of the schools (n=39, 49.4%) reported receiving an annual budget of $500 or more from their board to support efforts to improve the health of students, while over one third (n=28, 35.4%) of the remaining schools indicated they had not received any funding. Three schools reported annual budgets of less than $500, and the remaining 9 schools did not respond. About 65% (n=51) of schools reported their board provided support for staff time to be used for health promoting activities (e.g., for professional development, monitoring of policy compliance, etc.; 6 schools did not respond).
Support from outside organizations
Several (n=54, 68.4%) schools reported receiving support from their local Public Health Unit on healthy eating, and 35.4% (n=28) were supported on obesity and weight-related issues. Six schools did not receive any resources from their public health units. Support was most often in the form of providing information/resources/programs (e.g., posters, toolkits; n=60, 75.6%), and roughly one third (n=28, 35.4%) of schools had developed or implemented programs with their local public health unit.
Many schools indicated they had worked with other organizations to promote health-related activities in the past year, including: non-governmental organizations (e.g., Canadian Cancer Society, Health and Stroke Foundation, Canadian Diabetes Association; n=49, 62.0%), Parks and Recreation Departments (n=21, 26.6%), youth organizations (n=24, 30.4%), health or fitness clubs (n=36, 45.6%), and board/division/district itinerant teachers (e.g., consultants, specialists, n=23, 29.1%).
Staff training on nutrition and promoting healthy body image
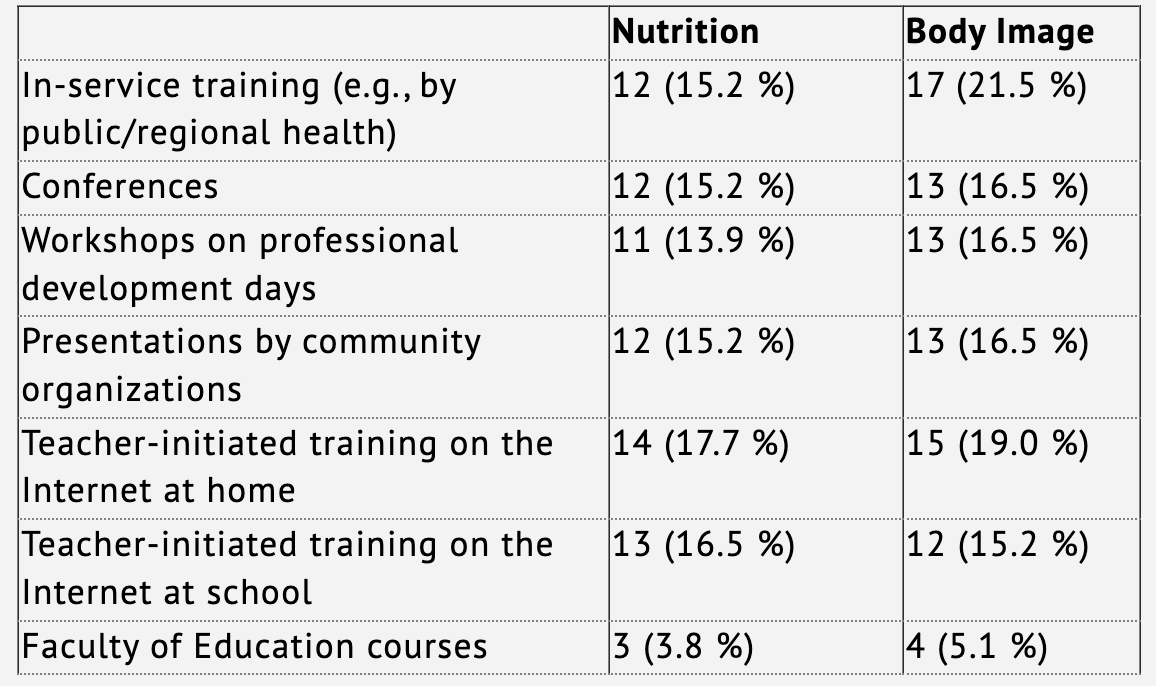
Over half of the schools surveyed indicated school staff had not received any form of training on nutrition (n=49, 62.0%) or promoting healthy body image (n=43, 54.4%) over the past year. See table 1 for the forms of training reported by schools.
In response to the question “does school staff have clear guidelines to refer students with suspected eating disorders to the appropriate health professional or community agency?”, 68.4% (n=64) replied yes, and 6.3% (n=5) were unsure (3 responses missing or uncodeable).
Staff training and resources provided by the school board
Two dichotomized variables for training on nutrition and on promoting healthy body image were computed in order to compare all those schools who had reported at least one form of training from the types listed in Table 2 (excluding teacher-initiated) to schools in which teachers had not received any nutrition or body image training.
As expected, schools that reported staff had received some form of training (e.g., in-service, conferences, workshops, presentations by community organizations, and/or Faculty of Education courses) on nutrition were more likely to report they had also been trained on promoting healthy body image (Chi-square = 32.9349, p < 0.0001).
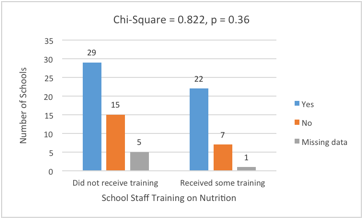
Next, chi-square analyses were performed to test whether staff training on nutrition and body image differed according to whether or not schools were provided with resources for health promotion activities from their boards (i.e., budget and support for staff time; See Figures 1-4). No significant differences were found, although a number of schools did not respond to the budget and staff time survey questions (9 and 7, respectively).
Figure 1. School Staff Trained in the Promotion of Healthy Body Image by Annual School Budget for Health Promotion Provided by School Board
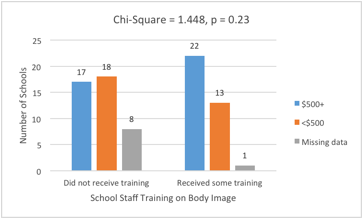
Figure 2. School Staff Trained in Nutrition by Annual School Budget for Health Promotion Provided by School Board
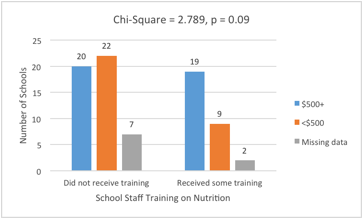
Figure 3. School Staff Trained in the Promotion of Healthy Body Image by School Board Support for Staff Time
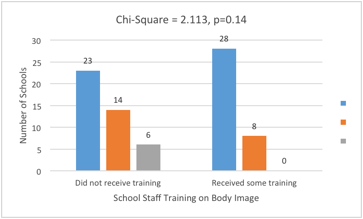
Figure 4. School Staff Trained in Nutrition by School Board Support for Staff Time
Discussion
Several experts have called for better education of teachers on health and weight-related issues to help minimize potential risks of encouraging weight bias, body preoccupation, and unhealthy weight-control behaviours among young persons (Pinhas et al., 2013; Russell-Mayhew et al., 2012; Yager, 2010; McVey et al., 2005; Weight Bias Summit, 2015); yet these appeals appear to not yet be consistently addressed based on the results of the current study. Over half of the schools surveyed reported that staff had not received any training on nutrition or body image over the past year. Among the few schools that reported nutrition-related training, the most common type was done on the internet and initiated by teachers. This finding suggests that teachers are interested in developing their skills on the matter, as shown in previous studies (Neumark-Sztainer et al., 1999; Yager, 2010; Yager & O’Dea, 2005). Further detail on the internet training completed by these teachers is not known. While various reputable resources have recently and continue to be made available electronically, with the vast amount of false health and nutrition information on the internet, it is essential to ensure educators are referring to evidence-based material.
On a positive note, several schools had received information on healthy eating from their local public health units and partnered with outside groups in delivering health promotion activities. Collaborations to support health initiatives are generally encouraged (Ontario Ministry of Education, 2015), although cautious consideration of the appropriateness of certain organizations is advisable. For instance, nearly half of the schools surveyed had worked with health or fitness clubs in the past year, which tend to be appearance and weight loss oriented, conflicting with recommendations for health programs targeting youth (Ontario Ministry of Education, 2015; Pinhas et al., 2013; Yager & O’Dea, 2005). For instance, in a newly released report on obesity and eating disorder prevention in adolescents, the American Academy of Pediatrics advises a focus on healthy lifestyle and body image, and discourages weight talk and the promotion of dieting (Golden, Schneider, Wood, & AAP Committee on Nutrition, 2016).

Along with teacher training and resources, past reports have cited limited resources, support from executives, and time among the primary barriers to implementing school-based health promotion programs (Belansky et al., 2009; Lister-Sharp et al., 1999). Results of the current study indicate a considerable disparity in resources provided by school boards for health promotion activities. Almost 40% of the schools surveyed reported a budget of over $1,000 annually, while a comparable proportion (35.4%) did not receive any financial support from their board. Also, a similar amount (27.9%) indicated their board had not allocated resources to permit staff time to pursue professional development and monitor health promoting programs and policies. In Ontario, funding for education is largely based on school enrollment, and as a result, schools in smaller towns or rural areas can be at a disadvantage (People for Education, 2016). Participation in training did not differ significantly by school budget or staff time resources, although this null finding may be due to the number of schools included in the analysis.

Schools were also asked whether staff had clear guidelines for referring students with suspected eating disorders. While over two thirds of the sample indicated procedures were in place, room for improvement remains given the importance of early intervention. Reviews of obesity prevention programs have found little indication of unhealthy weight-control behaviours occurring post intervention (Carter & Bulik, 2008; Waters et al., 2011); nonetheless, among predisposed students, some case studies suggest nutrition curriculum can trigger the onset of eating disorders (Pinhas et al., 2013). In such instances, it is essential that health and physical education teachers are competent at recognizing the signs, or know when to consult a health professional. The Ontario Ministry of Education’s (2013) Supporting Minds document instructs teachers to refer students struggling with eating disorders or other mental health concerns to guidance counsellors. While a recent scan found the large majority of Ontario secondary schools now have a guidance counsellor, results indicated student access vary considerably, with ratios of nearly 600 students to one counsellor reported in some schools (Hamlin, Cameron, & Watkins, 2016). Moreover, inconsistencies and uncertainties of the role of guidance counsellors was evident, with many expected to support youth in several diverse areas requiring complex skills (Hamlin et al., 2016; People for Education, 2016). Likewise, Yager and O’Dea (2007) express concerns about confusion among school personnel regarding their role in youth obesity and eating disorders. Schools represent a key setting for prevention and health promotion efforts, but are not equipped for activities bordering on treatment (Yager & O’Dea, 2007), and hence the importance of emphasizing the use of proper referral procedures.
Others may debate whether school-wide guidelines on eating disorders, and staff training on nutrition and body image, are necessary or reasonable, as these issues are among many health concerns. Indeed, it is prudent to remember the logistical realities of the school context when interpreting results and in making recommendations for school-based health strategies. A marked disconnection appears to exist between the expectations from above and current school-level capacities (Hamlin et al., 2016; People for Education, 2016). Schee and Gard (2014) question the added obligation of teachers to be health role models and facilitators, advising for more dialogue amongst policy makers, educators, and health workers.
Conclusion
Conclusions of the study are primarily limited by the sample size and representativeness. However, while 79 schools were surveyed, staff at these institutions could potentially impact over 50,000 enrolled students in single year. A number of other limitations merit acknowledgement. For instance, results were dependent on the knowledge of the school representative filling out the survey. It is plausible that the representative was not fully aware of all professional development activities and resources accessed by teachers or provided to the school. In addition, the survey did not assess individual teachers’ perceptions of support, actual health-related knowledge and views, or performance in teaching health curriculum. Moreover, the effectiveness of the training that some teachers received is unknown. Encouragingly, professional development workshops have been shown to improve teachers’ self-efficacy in delivering health and nutrition initiatives and in the prevention of eating disorders (Snelling, Ernst & Belson, 2013; McVey, Gusella & Tweed & Ferrari, 2009). Also, weight bias interventions appear promising based on early evidence, although repeated exposure may be required for sustained changes (McVey et al., 2013).
This paper provides a glimpse of the current situation regarding teacher preparedness to effectively and safely deliver health promotion programs and curriculum to secondary school students. In the new Ontario health curriculum (2015), educators are advised to increase their skills and reflect on their own health-related biases and values by seeking out training opportunities. Correspondingly, Principals are held responsible for facilitating teachers’ participation in professional development activities, and partnering with the school board and public health units. However, to date, teachers appear to have predominately relied on material resources from public health units. Additional consideration of the available resources, support, and preparation of educators is advisable in order to ensure the effective delivery of the new health curriculum, and continuing school-based health promotion and obesity prevention efforts.
References
Belansky, E.S., Cutforth, N., Delong, E., Ross, C., Scarbro, S., Gilbert, L., et al. (2009). Early impact of the federally mandated Local Wellness Policy on physical activity in rural, low-income elementary schools in Colorado. Journal of Public Health Policy, 30(Suppl 1), S141–60.
Bredin, C., Thompson-Haile, A. & Leatherdale, S.T. (2015). Supplemental Sampling and Recruitment of Additional Schools in Ontario: Technical Report Series. Waterloo, Ontario: University of Waterloo, 3(2).
Carter, F. A., & Bulik, C.M. (2008). Childhood obesity prevention programs: how do they affect eating pathology and other psychological measures? Psychosomatic Medicine, 70, 363-371.
Chen, Y-H., Yeh, C-Y., Lai, Y-M., Meei-Ling, S., Huang, K-C. & Chiou, H-Y. (2010). Significant effects of implementation of health-promoting schools on schoolteachers’ nutrition knowledge and dietary intake in Taiwan. Public Health Nutrition, 13(4), 579-588.
Golden, N.H., Schneider, M., Wood, C., & AAP Committee on Nutrition (2016). Preventing obesity and eating disorders in adolescents. Pediatrics, 138(3), e20161649.
Greenleaf, C., Martin, S. B., & Rhea, D. (2008). Fighting fat: how do fat stereotypes influence beliefs about physical education? Obesity, 16(Suppl 2), S53-59.
Greenleaf, C. & Weiller, K. (2005). Perception of youth obesity among physical educators. Social Psychology of Education, 8, 407-423.
Kropski, J.A., Keckley, P.H., & Jensen, G.L. (2008). School-based obesity prevention programs: an evidence-based review. Obesity, 16(5), 1009-1018.
Leatherdale, S.T., Brown, K.S., Carson, V., Childs, R.A., Dubin, J.A., Elliott, S.J., Faulkner, G., Hammond, D., Manske, S., Sabiston, C. M., Laxer, R.E., Bredin, C., Thompson-Haile, A. (2014). The COMPASS study: a longitudinal hierarchical research platform for evaluating natural experiments related to changes in school-level programs, policies and built environment resources. BMC Public Health, 14, 331.
Lister-Sharp, D., Chapman, S., Stewart-Brown, S., & Sowden, A. (1999). Health promoting schools and health promotion in schools: Two systematic reviews. Health Technology Assessment, 3(22), 1-207.
McVey, G.L., Gusella, J., Tweed, S. & Ferrari, M. (2009). A controlled evaluation of web-based training for teachers and public health practitioners on the prevention of eating disorders. Eating Disorders: Journal of Treatment and Prevention, 17(1), 1-26.
McVey, G. L., Tweed, S., & Ferrari, M. (2005). The role of teachers in the prevention of eating disorders: Findings from a school-based prevention program. Poster presented at the Eating Disorder Research Society, Annual Meeting, Toronto, Ontario.
McVey, G.L., Walker, K.S., Beyers, J., Harrison, H.L., Simkins, S.W. & Russell-Mayhew, S. (2013). Integrating weight bias awareness and mental health promotion into obesity prevention delivery: a public health pilot study. [Erratum appears in Preventng Chronic Disease, 10. http://www.cdc.gov/pcd/issues/2013/12_0185e.htm.] Preventing Chronic Disease, 10, 120185.
Neumark-Sztainer, D., Story, M., & Harris, T. R. (1999). Beliefs and attitudes about obesity among teachers and school health care providers working with adolescents. Journal of Nutrition Education, 31(1), 3–9.
Ontario Agency for Health Protection and Promotion (Public Health Ontario). Addressing obesity in children and youth: evidence to guide action for Ontario. Toronto, ON: Queen’s Printer for Ontario; 2013.
Ontario Ministry of Education (2015). The Ontario Curriculum, Grades 9 to 12: Health and Physical Education. Available at: http://www.edu.gov.on.ca/eng/curriculum/secondary/health9to12.pdf (Accessed March 11, 2016).
Pan Canadian Joint Consortium for School Health: Healthy School Planner; 2014. http://hsp.uwaterloo.ca/).
Peterson, J.M., Puhl, R.M., & Luedicke, J. (2012). An experimental assessment of physical educators’ expectations and attitudes: the importance of student weight and gender. Journal of School Health, 82(9), 432-440.
People for Education (2016). The geography of opportunity: what’s needed for broader student success. Annual Report on Ontario’s Publicly Funded Schools. Toronto: People for Education.
Pinhas, L., McVey, G., Walker, K.S., Norris, M., Katzman, D., & Collier, S. (2013). Trading health for a healthy weight: the uncharted side of healthy weights initiatives. Eating Disorders: The Journal of Treatment & Prevention; 21(2), 109-116.
Puhl, R.M. & Heuer, C.A. (2010). Obesity stigma: Important considerations for public health. American Journal of Public Health, 100, 1019-1028.
Russell-Mayhew, S., McVey, G., Bardick, A., & Ireland, A. (2012). Mental health, wellness, and childhood overweight/obesity. Journal of Obesity, article ID 281801, 9 pages.
Schee, C. V., & Gard, M. (2014). Healthy, happy and ready to teach, or why kids can’t learn from fat teachers: the discursive politics of school reform and teacher health. Critical Public Health, 24(2), 210-225.
Sharma, S., Dortch, K.S., Williams, C.B., Truxillio, J.B., Rahman, G.A., Bonsu, P., & Hoelscher, D. (2013). Nutrition-related knowledge, attitudes, and dietary behaviors among Head Start Teachers in Texas: A cross-sectional study. Journal of the Academy of Nutrition and Dietitics, 113(4), 558-562.
Snelling, A.M., Belson, S.I., & Young, J. (2012). School health reform: investigating the role of teachers. The Journal of Child Nutrition & Management, 36(1), n1.
Snelling, A.M., Ernst, J., & Belson, S.I. (2013). Teachers as role models in solving childhood obesity. Journal of Pediatric Biochemistry, 3, 55-60.
Thompson-Haile, A. & Leatherdale, S.T. (2013). School Board and School Recruitment Procedures. COMPASS Technical Report Series. Waterloo, Ontario: University of Waterloo, 1(3).
Tremblay, M., Shields, M., Laviolette, M., Craig, C.L., Janssen, I., & Connor Gorber, S. (2010). Fitness of Canadian children and youth: results from the 2007–2009 Canadian Health Measures Survey. Health Reports, 21, 1–7.
Waters, E., de Silva-Sanigorski, A., Burford, B.J., Brown, T., Campbell, K.J., Gao, Y., Armstrong, R., Prosser, L. & Summerbell, C.D. (2011). Interventions for preventing obesity in children. Cochrane Database of Systematic Reviews, Issue 12, Art. No.: CD001871.
Weight Bias Summit (2015). Available at: http://www.obesitynetwork.ca/files/Weight_Bias_Summit-_Full_Summary-_Sep_2015_final.pdf (Accessed: March 11, 2016).
Yager, Z. (2010). Issue of teacher training in the prevention of eating disorders and childhood obesity in schools. Chapter 5 in Childhood Obesity Prevention: International Research, Controversies, and Interventions. Eds. O’Dea, J. A., & Erikson, M. Oxford University Press Inc., New York.
Yager, Z., Diedrichs, P. C., Ricciardelli, L. A., & Halliwell, E. (2013). What works in secondary schools? A systematic review of classroom-based body image programs. Body Image, 10, 271-281.
Yager, Z. & O’Dea, J.A. (2005). The role of teachers and other educators in the prevention of eating disorders and child obesity: what are the issues? Eating Disorders, 13(3), 261-278.
Yager, Z. & O’Dea, J. (2009). Body image, dieting and disordered eating and activity practices among teacher trainees: implications for school-based health education and obesity prevention programs. Health Education Research, 24(3), 472-482.
Yager, Z. & O’Dea, J. (2015). School-based prevention. In: Smolak, L., Levine, M.P. (Eds.). The Wiley Handbook of Eating Disorders. John Wiley & Sons, Ltd.
Authors








